
BY GENEVIEVE MULLINS
Cancer diagnosis in itself presents immediate challenges and stressors for patients; often resulting in the neglect of preparing for the late effects following treatment. With the advancement in treatment and subsequent increased survival rates, quality of life after therapy is – now more than ever – of particular importance. One of the key survivorship concerns after cancer treatment is the risk for infertility. Chemotherapy, radiation and surgery are the most frequent determinants of infertility among cancer survivors.
Chemotherapy
Most chemotherapeutic drugs are considered to be toxic to the gonads, resulting in temporary or permanent disruption to reproductive organs and glands that control fertility. Alkylating agents are the primary chemotherapeutic agents associated with the highest risk of permanent infertility.
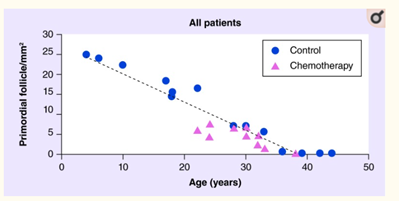
A quantitative study examined the effects of alkylating agents on the ‘reproductive lifespan’ (known as ovarian reserve) among female cancer patients. Out of the 26 patients, ten received chemotherapy (with alkylating regimens) while 16 did not (control group). Though age is a significant determinant of ovarian reserve, the results found that chemotherapy significantly diminishes the number of follicles – containing egg cells – compared with the control group.
Women who have had chemotherapy before or during their planned family must be aware that chemotherapy can lead to premature ovarian failure, i.e., menopause occurring earlier than it otherwise would have. In other words, the biological clock for starting a family now may have a shorter time to run, and stop at an earlier age than expected.
One of the main concerns men face when undergoing chemotherapy, is the damage to sperm production. As cancer is designed to kill rapidly dividing cells, this in turn results in both cancerous cells and healthy sperm cells being destroyed. Results from a study reported 37% of male patients having complete absence of sperm in seminal fluid (known as Azoospermia) after chemotherapy. This does tend to recover over time, particularly in younger men. Men who have had chemotherapy should never assume they may not be fertile; they should be tested for viable sperm and if negative, retested later on usually after a year or so.
Radiation
Radiation therapy uses high doses of energy x-rays to kill cancer cells. Like chemotherapy, radiation is designed to kill rapidly dividing cells, resulting in the temporary or permanent damage to reproductive cells. Radiation directly targeted at the testicles/ovaries, or lower bodily region, can affect a patient’s reproductive system.
Radiation shielding is a technique used when radiation is given to the abdomen or pelvis. Small lead shields are placed over the ovaries/testicles and other parts of the reproductive system to reduce the amount of radiation exposure they receive.
Secondary (indirect) testicular or ovarian failure can occur as a result of radiation therapy to the brain. More specifically, radiation may lead to a disruption in the functioning of hormonal regions in the brain; the hypothalamus and pituitary gland. The two work together to produces hormones (luteinizing hormone and follicle-stimulating hormone) needed for normal sexual function.
Surgery
Surgery might be the chosen cancer treatment when a tumor is present in the ovaries/ testicles or nearby abdominal or pelvic organs. Tumors that exist near the nervous system, such as the brain or spinal cord may also affect a patient’s fertility.
Fertility preservation
The effects of cancer treatment on reproductive functioning should be discussed before initiating treatment. The American Society of Clinical Oncology (ASCO) seeks to provide evidence-based clinical guidelines on fertility preservation, stating that “health care providers should address the possibility of infertility with patients treated during their reproductive years or with parents/guardians of children and be prepared to discuss possible fertility preservation options’.
Women fertility preservation
Fertility preservation options for women include egg freezing, embryo freezing and ovarian tissue freezing.
Egg freezing (oocyte cryopreservation) – An established and successful technique of storing a woman’s unfertilized eggs. Once ready to be used, they will be thawed and fertilized with sperm. When the fertilized egg develops into an embryo, a simple procedure is undertaken to transfer the embryo into your uterine cavity. This method may mean delaying cancer treatment until eggs can be collected at an appropriate time in the woman’s menstrual cycle.
Embryo freezing (Embryo cryopreservation) – Eggs are removed from the patient and fertilized in a test tube with the sperm of a partner or donor. The resulting embryos are then frozen and stored.
Ovarian tissue freezing – Involves the process of freezing and storing tissue from the ovarian cortex. When you are ready to start a family, the tissue containing undeveloped eggs can be reimplanted. This method is considered less proven at this time, but the procedure can be performed urgently if necessary, to allow cancer treatment to start. Many haematology and oncology units give depot injections of gonadotrophin releasing hormone analogues to suppress ovary function during treatment; there is some evidence that this may help protect the ovaries from chemotherapy damage.
Men fertility preservation:
Fertility preservation options for men most commonly include sperm banking:
Sperm banking (Cryopreservation) – Before initiating cancer therapy, sperm banking is a strongly recommended procedure, as a single treatment session can significantly impact the quality of the sample and sperm DNA integrity. The technique of intracytoplasmic sperm injection (ICSI) allows the successful freezing and future use of a very limited amount of sperm.
Consult your doctor or fertility specialist
The damage to reproductive organs is determined by drug dosage, type, and the age and gender of the patient. Infertility can be temporary, last months to years, or permanent.
If you are preparing for cancer treatment and want to preserve your fertility, speak with a doctor or fertility specialist for the options that may be available to you. If fertility preservation is not a desirable or feasible option, there are other viable alternatives for becoming a parent, such as donor egg or sperm, surrogacy, or adoption.
Genevieve’s fascination with the mind and its impact on human behavior led her to pursue a Bachelor of Psychology, at QUT, and then further continued to complete an honours degree, at University of Sunshine Coast. Genevieve envisions her future to embrace a career assisting adults in discovering the cause of psychological issues and in turn providing guidance to alleviate pain and suffering. When she’s not working full time, Genevieve can be found relaxing at a coffee shop, jogging along the boardwalk of the Brisbane River, partaking in an early morning yoga class, or simply reading a good novel with a cup of tea.





